Uterine fibroids
What are uterine fibroids?
Fibroids are the most common benign tumors in women and originate in the muscular wall of the uterus. It is estimated that approximately 7 out of 10 women will have fibroids at some point during their lifetime. However, their prevalence is 8 to 10% between the ages of 30 and 40.
It is scarce for them to become malignant tumors that can be life-threatening to the woman who suffers from them. However, they can affect a woman’s health in other ways. Fibroids can cause abnormal and heavy vaginal bleeding; they can grow to a significant size and cause symptoms of pain and discomfort by compressing other organs in the female pelvis, such as the bladder and the intestine. Fibroids can affect the uterus, interfering with the normal reproduction process and the ordinary course of pregnancy. One in four women with infertility may have uterine fibroids. However, they are responsible for only 2-3% of infertility cases if other causes are excluded.
How might uterine fibroids affect a woman's fertility?
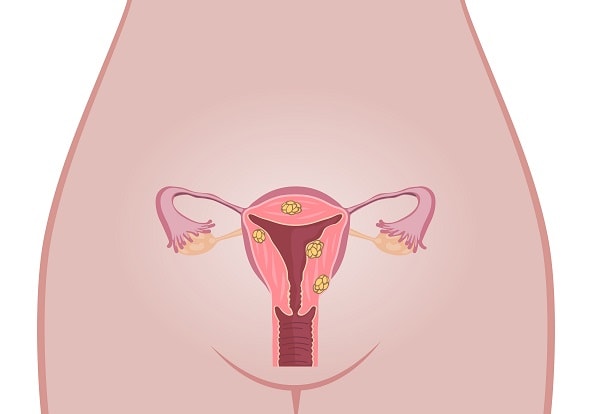
Fibroids can decrease a woman’s chances of becoming pregnant and carrying her pregnancy to term due to different factors. The most relevant of these is their location. Fibroids can grow from the wall of the uterus outward (subserosal fibroids), in the thickness of the uterine wall (intramural fibroids), or from the wall of the uterus into the uterine cavity (submucosal fibroids).
There is enough medical evidence to say that subserosal does NOT decrease the possibility of getting pregnant naturally, nor does it affect the pregnancy’s development.
On the other hand, because they enter the uterine cavity, submucous fibroids create a hostile environment that interferes with embryo implantation and development; therefore, most medical authors and scientific publications agree that submucous fibroids decrease the chance of pregnancy and increase the risk of spontaneous pregnancy loss (miscarriage).
There is relevant controversy about whether intramural fibroids affect the ability to become pregnant and the potential for pregnancy development. This only occurs when the fibroids are larger than 4.5 to 5 cm or when they are multiple.
How is the diagnosis for uterine fibroids made?
There are several ways to study the presence of fibroids in a woman’s uterus. The initial approach is a medical consultation in which the symptoms that raise suspicion of the existence of fibroids are investigated. A clinical examination by the gynecologist is also especially important because abnormalities in the size and contours of the uterus can be detected, which are also suggestive of the disease.
Furthermore, the transvaginal ultrasound allows the presence and size of fibroids to be evaluated with great sensitivity. At times, other complementary studies can perform a more thorough examination of the uterine cavity or adjacent structures, but they are rarely required.
What does the treatment of uterine fibroids consist of?
Suppose fibroids are affecting the woman’s quality of life or the possibility and prognosis of pregnancy. In that case, they can be removed by surgery, always to carry out, as far as possible, minimally invasive and outpatient procedures.
Hysteroscopy, which consists of inserting a small lens into the uterine cavity, allows the physician to see the uterus’s inside on a real-time video screen. The physician can insert small forceps to remove submucosal fibroids. It is the first method of choice to treat lesions that affect the uterine cavity and, in trained hands, has an extremely low incidence of complications.
Laparoscopy is based on entering a lens into the abdominal cavity through a small incision of 1 cm or less in the navel and some instruments or forceps through minimal incisions (0.5 cm) in the lower abdomen. This technique removes subserosal and intramural fibroids and has a minimal incidence of postoperative pain, with rapid recovery and minimal time of disability.
It must be understood that most patients with myomatosis do not present symptoms and do not require any treatment. However, in women who have difficulty getting pregnant and have large submucous or intramural myomas, surgical treatment is simple, minimally invasive, and achieves excellent results.